
This post was reviewed for medical accuracy by Rosalie Gunson, a Certified Registered Nurse Practitioner specializing in fertility care.
If your last pregnancy ended with a D&C, you may be wondering how long you should wait before trying again, and whether the procedure had any impact on your ability to get pregnant again.
Most doctors recommend waiting to start TTC again at least one full cycle after a D&C, although you can technically get pregnant again as soon as you ovulate. The procedure can affect the timing of your next cycle, but it’s unlikely to lead to any lasting fertility problems.
D&Cs can be done electively to end unwanted pregnancies in the first trimester. However, since this is a fertility blog, this post focuses on D&Cs in the context of miscarriage and wanted but non-viable pregnancies.
What is a D&C, anyway?
D&C stands for dilation and curettage. It’s a quick outpatient surgical procedure in which tissue is removed from the uterus.
The “dilation” part of a D&C refers to dilation of the cervix, similar to the dilation that happens during labor. The cervix just has to widen enough for the instrument to pass through, though — it’s nowhere near large enough for a baby!
The word “curettage” sounds a bit like cutting, but nothing is cut during a D&C. It’s called that because tissue is scraped from the uterus using a spoon-like instrument called a curette. Suction may also be used.
Why would someone get a D&C?
You may have heard of D&C’s in the context of abortion, but there are other reasons for the procedure, including:
- Removal of fetal tissue, if not expelled by the body during a first-trimester miscarriage (may be called a missed or incomplete miscarriage)
- Removal of small pieces of the placenta, if not expelled by the body during childbirth
Letting this “leftover” tissue in the uterus can lead to heavy bleeding and infection, so it’s important to get it out.
Tissue may be removed during a D&C so it can be tested. Fetal tissue can be tested for chromosomal abnormalities that might explain the loss of the pregnancy. That’s more likely to be done if this was not your first miscarriage.
You don’t actually need to be pregnant in order to have a D&C. For example, sometimes the procedure is done to collect endometrial tissue to test for cancer, if the results of a less invasive biopsy were not conclusive.
Do all miscarriages require a D&C?
No. A D&C is done in only about half of miscarriages.
That’s because the majority of miscarriages happen at the beginning of the first trimester, when the fetus is incredibly tiny. The body usually clears things out on its own, or with the help of an oral medication like misoprostol.
A D&C may be needed when the pregnancy is a bit more established, usually in the ballpark of 10 to 14 weeks.
Choosing a D&C rather than waiting for miscarriage
Sometimes the body doesn’t get the signal that the fetus is no longer alive. You may have seen this scenario called a “missed miscarriage.” With a missed miscarriage, there may be no obvious sign that anything is wrong. It is often discovered when the doctor can’t find a heartbeat at a prenatal visit.
If your doctor has diagnosed a missed miscarriage, or it’s clear that the pregnancy is not viable, you may be given the choice between waiting for a natural miscarriage, taking medication such as misoprostol, or scheduling a D&C. That is obviously a very personal and gut-wrenching decision, but here are a few advantages of each option:
Choosing to wait for a miscarriage (with or without misoprostol):
- You can process the loss over time.
- You’ll be able to stay in the privacy of your home.
- There are always lots of good reasons for avoiding surgery if you can.
Choosing to have a D&C:
- There will be a clear end date. Waiting for a miscarriage to take place over days or weeks can be emotionally devastating.
- You can avoid the pain and discomfort of an ongoing miscarriage (misoprostol can cause very strong cramps, but even a med-free miscarriage can be painful and traumatizing)
- You won’t see fetal tissue.
- Even if you wait, you may end up needing a D&C anyway. Doing the surgery now will ensure that there is no tissue left behind.
Fertility nurse Rosalie Gunson, RN says that in her experience, the D&C is often preferable in the end:
“One thing that I did not realize until I worked in a fertility clinic is how when the doctor gives patients options like 1) expectant management, 2) medication, or 3) D&C, the D&C sounds scary and like the worst option,” she says. “Of patients that have done expectant management and medication, most will tell you they would choose the D&C right away if they had to do it again. Almost every patient I’ve had wishes they did not do medication (miso) because the pain is INTENSE, and bleeding is way more than most people ever expected. It sounds natural but it’s far from comfortable and typically traumatic, even when we give Percocet and nausea meds.” – Rosalie Gunson, RN
When can you expect your next period after a D&C?
A D&C will affect your menstrual cycle because it involves the removal of the uterine lining, which is shed during your period. Your next period could arrive as much as 6 weeks after your D&C procedure.
As with any surgery, there’s a small chance of developing an infection after a D&C. A little bit of spotting or cramping after a D&C is normal, but see your doctor if you have heavy bleeding, severe abdominal pain, or a fever afterwards.
If you do get bleeding, use pads rather than tampons to prevent infection. You should definitely avoid sex until you are no longer bleeding.
How soon after a D&C can you try to get pregnant again?
You may need time to process your experience and grieve before contemplating another pregnancy, and that’s totally normal. Miscarriage can be traumatic at any stage of pregnancy, so you should absolutely take all the time you need.
If you do feel ready right away, most doctors recommend waiting until you have at least one regular period before starting TTC again. Some doctors actually recommend waiting at least three months after any miscarriage.
The idea is that waiting gives your uterus a chance to prepare for a new pregnancy, but there’s nothing especially dangerous about getting pregnant very soon after a D&C. (For more info about the importance of a good uterine lining for conception, see this post.)
Does a D&C affect your future fertility?
You may wonder if having a miscarriage in general, or a D&C specifically, will make you infertile in the future.
Having had one miscarriage doesn’t necessarily mean you’re more likely to have a second one. Lurking in fertility forums may give you the impression that recurrent pregnancy loss is super common, but it’s really not common at all!
In fact, most miscarriages are due to random flukes in the fetus’ very early development. After one miscarriage your odds of conceiving again within a year are high, especially if you are relatively young and you didn’t have issues conceiving before.
If this wasn’t your first loss or you struggled to conceive to begin with, you may want to consult with a reproductive endocrinologist (RE) before trying again.
You and your partner may be sent for testing, if it wasn’t done before. That could include an HSG for you (I have a whole post about that test here), and a sperm analysis for your partner.
As for the D&C itself, the procedure probably won’t affect your fertility unless there was some sort of complication during the surgery.
For example, scar tissue in the uterus can lead to Asherman’s Syndrome. But this is a pretty rare occurrence — most of the time, a D&C does not impact future fertility at all. (And even if you did develop scar tissue, doctors may be able to surgically remove it.)
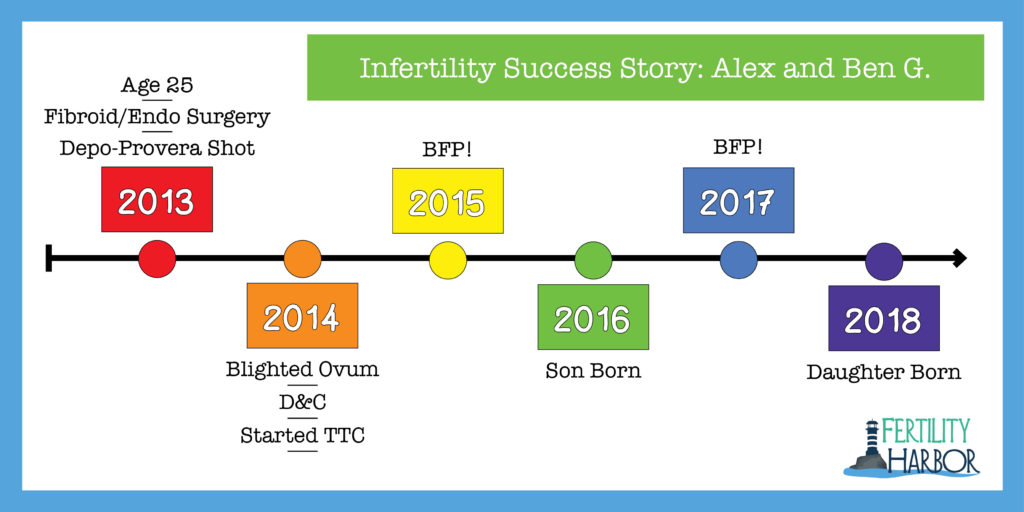
Infertility Success Story: Alex and Benjamin G.

My friend Alex had a D&C at about 6-8 weeks. (She had recently come off the Depo-Provera shot and hadn’t had a period since, so she wasn’t sure of the exact date.)
Her hCG levels were not doubling as expected, so she had an ultrasound. The scan showed that the sac was empty — there was no fetus developing. It was a blighted ovum.
She was offered a choice between waiting for the miscarriage to happen naturally or having a D&C.
She was driving for public transit at the time, and she didn’t want to have a miscarriage while stuck on a bus. She chose the D&C. Can’t say I blame her!
“I think knowing it was going to be over on a certain day was… not exactly comforting, but I was able to process it easier,” she says.
She and her husband began seriously trying about 4 months later, but it didn’t happen right away.
In fact, she was so obsessively TTC — including tracking her periods with an app, using ovulation predictor kits, etc. — that Alex believes stress kept her from conceiving.
Alex and her husband had decided that if they didn’t conceive within a year, they would look into adoption. They were not planning to pursue IVF or other fertility treatments.
As that milestone approached, they started talking about adoption more seriously. Alex stopped tracking everything… and got pregnant.
While it didn’t have a direct impact on her fertility issues, Alex does have a history of long, heavy periods and endometriosis.
About 6 months before the blighted ovum, Alex had surgery to remove a large fibroid at the back of her uterus. It turned out that the fibroid was surrounded by endometrial tissue, which was starting to attach to her small bowel.
Endometriosis doesn’t show up on an ultrasound, so it was a complete surprise to her and her doctors. Alex was told that if the endometriosis had been any worse, she would have needed a hysterectomy!
Thankfully, Alex hasn’t had any more painful fibroids or endometriosis-related problems since the surgery.
And after her son was born, her periods became much more regular. When she was one day late, she knew she was pregnant again!
(I’ve shared Alex’s photo and story with her permission, obviously!)
Conclusion
It’s physically possible to get pregnant very soon after a D&C — basically as soon as you begin ovulating again.
Emotionally, though, you may need more time to grieve the loss and consider your next steps. Take all the time you need, and remember to give yourself some grace, mama.
Resources for Further Reading:
Dilation and Curettage FAQ from American College of Obstetricians and Gynecologists (ACOG)
This post was written in 2020 with minor updates in 2025.
 I’m Jenn! Here I am with my beautiful twin boys. My pregnancy was possible thanks to fertility treatment for PCOS.
I’m Jenn! Here I am with my beautiful twin boys. My pregnancy was possible thanks to fertility treatment for PCOS.


